End-of-life care definition: hospice support in California

End-of-life care definition: hospice support in California
Over 1.5 million Americans receive hospice care each year, with more than 80% choosing to spend their final days at home surrounded by loved ones. For caregivers in California, understanding what end-of-life care truly means can transform confusion into confidence when supporting a terminally ill family member. This guide clarifies hospice definitions, eligibility requirements, services available at home, and how to access compassionate support that honors dignity and comfort during life’s final chapter.
Table of Contents
- Defining End-Of-Life Care: Medical And Legal Framework
- Core Components Of Hospice Services In Home-Based End-Of-Life Care
- Legal And Eligibility Criteria For Hospice Care In California
- Role And Support Of Caregivers In End-Of-Life Home Care
- Common Misconceptions About End-Of-Life And Hospice Care
- Comparing End-Of-Life Care To Palliative Care
- Benefits Of Hospice Care On Patient Comfort And Family Support
- Summary And Practical Steps For Accessing Hospice Care In California
- Find Compassionate Hospice Care In California With Graceland Hospice Care
- Frequently Asked Questions About End-Of-Life Care And Hospice In California
Key takeaways
| Point | Details |
|---|---|
| End-of-life care focuses on comfort | Medical care for patients with six-month prognosis emphasizing quality of life over cure. |
| Hospice teams provide holistic support | Nurses, doctors, social workers, and chaplains deliver pain relief and emotional care at home. |
| California requires legal certification | Physician certification and licensed providers ensure compliance and quality standards. |
| Caregiver education reduces stress | Training and support from hospice teams decrease anxiety and depression by 30-40%. |
| Early hospice enrollment maximizes benefits | Timely referral improves patient comfort and may reduce hospital admissions by 40%. |
Defining end-of-life care: medical and legal framework
End-of-life care represents a specialized approach to medical treatment when curative options no longer serve a patient’s best interests. The Medicare Hospice Benefit defines this care as services provided when a physician certifies a patient has six months or less to live if the illness follows its expected course. This prognosis threshold establishes eligibility for hospice programs nationwide, including California.
The legal framework requires two key components: physician certification and patient acceptance. A doctor must formally document the terminal prognosis based on clinical evidence and disease progression. The patient or their healthcare proxy must then agree to shift treatment goals from cure to comfort, acknowledging that hospice services will not pursue aggressive interventions aimed at reversing the underlying condition.
California’s approach aligns with federal Medicare standards while adding state-specific licensing requirements. Understanding what is end of life care helps families recognize when this transition becomes appropriate. The care philosophy centers on three pillars:
- Comfort-focused symptom management replacing curative treatments
- Dignity preservation through patient-centered care planning
- Quality of life enhancement during remaining time
This framework distinguishes hospice from other medical services. While emergency departments aim to stabilize and reverse health crises, hospice accepts death as a natural process requiring compassionate support rather than aggressive intervention. The Medicare hospice coverage structure provides comprehensive benefits including medications for symptom control, medical equipment, and interdisciplinary team services delivered primarily at home.
Legal protections ensure patients receive consistent, quality care regardless of where they live in California. State regulations mandate specific staffing levels, response times, and care coordination protocols that licensed hospice providers must follow.
Core components of hospice services in home-based end-of-life care
Hospice care at home involves far more than occasional nurse visits. The interdisciplinary team approach delivers comprehensive medical, emotional, and spiritual support through coordinated professionals working together. This team typically includes registered nurses who manage symptoms and medications, physicians who oversee medical care plans, social workers who address practical and emotional needs, chaplains who provide spiritual counseling, and home health aides who assist with daily activities.
Pain and symptom management stands as the highest clinical priority. Nurses assess discomfort levels regularly and adjust medications to achieve optimal relief while maintaining alertness when patients desire it. This specialized symptom control extends beyond pain to address nausea, breathing difficulties, anxiety, and other distressing conditions common in terminal illness.

The statistics reveal patient preferences clearly: approximately 80% of hospice care occurs in private homes rather than facilities. This preference reflects the profound comfort most people feel when surrounded by familiar settings and loved ones during their final weeks. Learning how to start hospice care at home empowers families to honor these wishes.
Psychosocial support addresses the emotional weight carried by both patients and families. Social workers help navigate advance directives, funeral planning, and grief counseling. Chaplains offer spiritual guidance respecting all faith traditions or secular worldviews. This holistic approach recognizes that dying involves more than physical decline.
The coordination among team members prevents fragmented care common in hospital settings. Weekly team meetings review each patient’s status, adjust care plans, and ensure family concerns receive attention. This integration means families work with one cohesive support system rather than juggling multiple disconnected providers.
Pro Tip: Request a team member contact list during your initial hospice meeting so you know exactly who to call for different needs, from medication questions to emotional support.
Families seeking comprehensive support can explore caregiver support hospice families resources that complement clinical services with practical guidance for the caregiving journey.
Legal and eligibility criteria for hospice care in California
California maintains rigorous licensing standards for hospice providers to protect vulnerable patients during their most dependent period. The California Department of Public Health oversees hospice licensing, requiring agencies to demonstrate compliance with continuous nursing availability and interdisciplinary oversight as mandated by state health and safety codes.
Eligibility hinges on three specific criteria that must be met before services begin:
- Terminal illness diagnosis with six-month or less prognosis if disease follows expected course
- Physician certification documenting the medical basis for prognosis determination
- Patient and family agreement to focus treatment on comfort rather than cure
The physician certification process requires detailed documentation. Two doctors typically review the case: the patient’s attending physician and the hospice medical director. They examine disease progression markers, recent hospitalizations, functional decline measures, and clinical indicators specific to the underlying condition. For cancer patients, this might include tumor spread and treatment failure. For heart failure, it could involve ejection fraction levels and medication response.
California law mandates that licensed hospice providers maintain 24-hour nurse availability for crisis intervention. This requirement ensures families never face emergencies alone, even at 3 a.m. Nurses must respond to urgent calls within one hour and arrive at homes within timeframes specified by care plans.
Regular interdisciplinary team reviews occur at least every 15 days to reassess patient needs and adjust services. These reviews examine pain control effectiveness, caregiver coping, and whether the care setting remains appropriate. If a patient stabilizes or lives beyond initial expectations, the team recertifies eligibility through updated physician assessments.
Compliance with these regulations protects families from substandard care while providing legal recourse if standards slip. Understanding how to start hospice care at home includes verifying a provider’s California license and accreditation status before enrollment.
The legal framework also addresses patient rights, requiring informed consent for all treatments and the right to revoke hospice services at any time to resume curative care.
Role and support of caregivers in end-of-life home care
Family caregivers form the backbone of successful home hospice care, providing daily support that enables patients to remain in familiar surroundings. Your role extends beyond basic caregiving to become an essential partner in the care team, implementing treatment plans and communicating changes in your loved one’s condition.
The emotional toll on caregivers cannot be understated. Watching a loved one decline while managing medications, personal care, and household responsibilities creates intense stress. Research shows that caregiver education reduces anxiety and depression by 30-40% through structured training and ongoing support from hospice professionals.
Hospice teams invest significant time educating caregivers on practical skills:
- Medication administration techniques and timing
- Positioning strategies to prevent bedsores and enhance comfort
- Recognizing signs of pain or distress requiring nurse assessment
- Understanding normal dying process changes to reduce fear
- Self-care practices preventing caregiver burnout
Early hospice referral maximizes the support benefits available to you. Enrolling when your loved one has months rather than days remaining allows time to develop trust with the team, learn necessary skills gradually, and access respite care services before exhaustion sets in. Delayed referrals force families to learn everything during the most emotionally intense period.
Your involvement in patient-centered planning ensures care reflects your loved one’s values and preferences. Hospice teams facilitate family meetings where everyone discusses goals, fears, and wishes for the remaining time. These conversations, while difficult, prevent confusion and conflict during crisis moments.
Pro Tip: Keep a dedicated notebook for tracking medication times, symptom changes, and questions for your nurse. This simple tool reduces mental load and ensures important details don’t slip through the cracks during stressful moments.
Exploring resources on the role of caregivers in hospice and understanding the role of hospice nurse orange county clarifies how professional support complements your family caregiving efforts.
Common misconceptions about end-of-life and hospice care
Misunderstandings about hospice care prevent many families from accessing timely support that could ease suffering. Correcting these myths empowers you to make informed decisions based on facts rather than fear.
The most damaging misconception claims hospice hastens death through medication or care withdrawal. Clinical evidence shows the opposite: hospice care extends life expectancy by reducing complications and hospitalizations through superior symptom management. Patients receiving hospice care often live longer than similar patients pursuing aggressive treatments that cause harmful side effects.
Many people believe hospice applies only during the final days or hours of life. This timing misunderstanding causes families to wait until crisis moments, missing months of potential support. Hospice eligibility begins when prognosis reaches six months or less, providing substantial time for meaningful support and quality of life improvements.
Confusion between hospice and palliative care creates additional barriers. While both prioritize comfort, understanding the differences hospice palliative care clarifies that palliative care can accompany curative treatments at any illness stage, while hospice requires accepting a terminal prognosis and forgoing cure-focused interventions.
Common myths requiring correction include:
- Myth: Hospice means giving up hope. Reality: Hope shifts from cure to comfort, meaningful time, and peaceful closure.
- Myth: Hospice is only for cancer patients. Reality: Any terminal diagnosis qualifies, including heart failure, dementia, and lung disease.
- Myth: Accepting hospice prevents hospital visits. Reality: Patients can seek emergency care if desired, though hospice aims to manage crises at home.
- Myth: Hospice costs create financial burden. Reality: Medicare, Medicaid, and most insurance plans cover hospice services completely.
These misunderstandings lead to delayed referrals that rob families of support during treatable symptom periods. When caregivers wait until the final 48 hours, they miss education opportunities, respite services, and emotional preparation that early enrollment provides.
Educating yourself through reliable sources like the hospice care overview prevents misconceptions from limiting your loved one’s comfort and your family’s wellbeing during this challenging time.
Comparing end-of-life care to palliative care
Distinguishing between hospice end-of-life care and palliative care helps you identify which service fits your loved one’s current needs and illness stage. While both philosophies prioritize comfort over cure, key differences in timing, treatment approach, and eligibility separate them.
End-of-life hospice care begins when a patient’s prognosis drops to six months or less and they choose to forgo curative treatments. At this point, all medical interventions aim solely at symptom relief and quality of life. Chemotherapy stops, dialysis ends, and aggressive cardiac interventions cease. The focus narrows completely to comfort measures, emotional support, and dignity preservation.
Palliative care offers greater flexibility. Patients can receive palliative services at any serious illness stage, even while pursuing treatments aimed at remission or cure. A cancer patient might continue chemotherapy while receiving palliative support for pain management and emotional counseling. This dual approach addresses suffering without requiring patients to abandon hope for disease reversal.
| Feature | End-of-Life Hospice Care | Palliative Care |
|---|---|---|
| Timing | Six months or less prognosis | Any stage of serious illness |
| Treatment approach | Comfort only, no curative care | Can combine with curative treatments |
| Eligibility requirement | Terminal diagnosis acceptance | Serious illness causing suffering |
| Insurance coverage | Medicare Hospice Benefit, most insurance | Variable coverage, often limited |
| Care location | Primarily home-based | Hospital, clinic, or home settings |
| Team composition | Full interdisciplinary hospice team | May be single specialist or limited team |
Understanding these distinctions prevents premature hospice referrals when palliative care better suits current needs. Conversely, it helps families transition to hospice at appropriate times rather than clinging to palliative services when prognosis and treatment burdens warrant comfort-focused care.
The differences hospice palliative care resources provide deeper exploration of when each service optimizes patient wellbeing. Many patients benefit from palliative care months or years before hospice becomes appropriate, creating a continuum of comfort-focused support throughout serious illness.
Both services share commitment to symptom management, patient autonomy, and family support. The primary distinction centers on treatment goals and prognosis timeframes rather than care quality or compassion levels.
Benefits of hospice care on patient comfort and family support
Clinical evidence demonstrates measurable improvements in patient outcomes and family wellbeing when hospice care replaces standard medical treatment during terminal illness. These benefits extend across physical comfort, healthcare utilization, and caregiver mental health domains.
Pain control data reveals significant disparities between care approaches. Studies show 78% of hospice patients report adequate pain control compared to just 55% receiving standard care. This 23-percentage-point gap reflects hospice expertise in complex symptom management and willingness to adjust medications aggressively for comfort rather than following conservative hospital protocols.
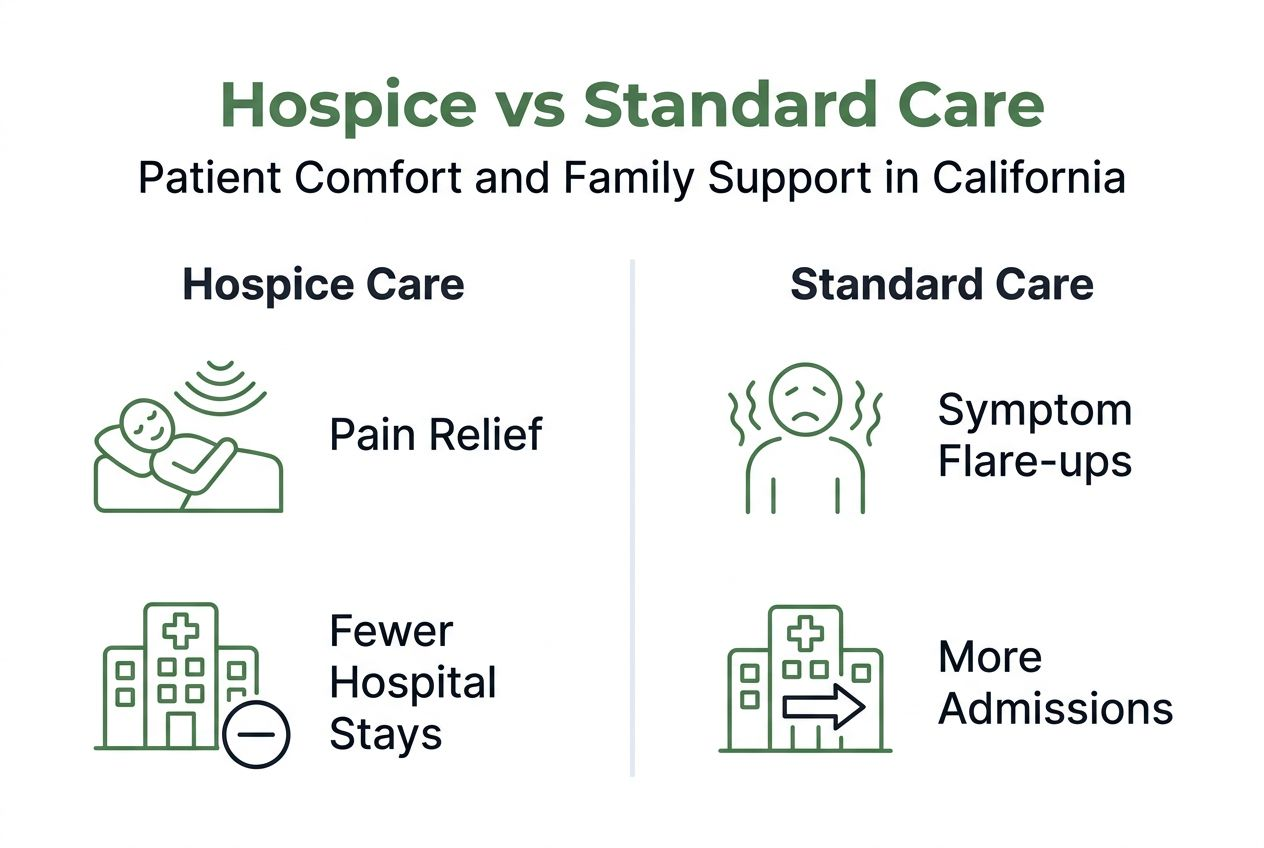
Hospitalization rates drop dramatically under hospice care. Patients enrolled in hospice experience up to 40% fewer hospital admissions during their final months compared to similar patients not receiving hospice services. This reduction spares families from disruptive emergency department visits, uncomfortable hospital stays, and the emotional toll of watching loved ones undergo futile interventions.
| Outcome Measure | Hospice Care | Standard Care |
|---|---|---|
| Adequate pain control | 78% | 55% |
| Hospital admission reduction | 40% decrease | Baseline |
| Caregiver anxiety reduction | 30-40% improvement | No improvement |
| Patient satisfaction | 95% family satisfaction | 70% satisfaction |
Caregiver mental health improvements represent equally important benefits. Family members supporting hospice patients report 30-40% reductions in anxiety and depression symptoms compared to caregivers managing terminal illness without hospice support. This improvement stems from education, respite care access, 24-hour nurse availability, and the emotional security of expert guidance.
The comprehensive support model addresses needs that standard medical care overlooks:
- Spiritual counseling helping families find meaning during loss
- Social work assistance with advance directives and funeral planning
- Bereavement support extending 13 months after death
- Medical equipment delivery removing logistical burdens
- Medication provision covering all comfort-related prescriptions
Pro Tip: Enroll in hospice as soon as eligibility criteria are met rather than waiting until the final weeks. Early enrollment allows time to build relationships with your care team, access educational resources before crisis moments, and utilize respite services preventing caregiver burnout.
Families seeking detailed outcome information can review the end of life care guide compassionate at home support which explores evidence-based benefits of comprehensive hospice services.
Summary and practical steps for accessing hospice care in California
Navigating the hospice enrollment process requires understanding specific steps that move your family from initial consideration to active care receipt. This systematic approach ensures compliance with California requirements while securing timely support.
-
Recognize eligibility indicators suggesting six-month or shorter prognosis. These include multiple hospitalizations within six months, progressive functional decline, weight loss despite adequate nutrition, and disease-specific markers your physician can identify.
-
Initiate conversation with your loved one’s primary physician or specialist. Request formal prognosis assessment and ask whether they believe hospice criteria are met. Physicians sometimes hesitate to suggest hospice, so you may need to raise the topic directly.
-
Obtain physician certification documenting the terminal prognosis and medical justification. This certification typically requires the attending physician and hospice medical director to review records and sign formal eligibility paperwork.
-
Discuss hospice care with your loved one and family members. Ensure the patient understands that accepting hospice means choosing comfort over curative treatments. This conversation, while difficult, prevents confusion and conflict later.
-
Research licensed California hospice providers serving your area. Verify state licensing through the California Department of Public Health website and check for Medicare certification if applicable to your insurance situation.
-
Contact selected hospice agencies to request initial assessments. Most providers offer free consultations where nurses visit your home, evaluate needs, explain services, and answer questions before you commit.
-
Review and sign hospice election paperwork once you select a provider. This documentation formalizes your choice to receive hospice benefits and establishes the care plan framework.
-
Coordinate with your existing healthcare team to ensure smooth transitions. Your hospice social worker typically manages communication with hospitals, specialists, and pharmacies to prevent service gaps.
-
Establish medication and equipment delivery logistics with your hospice provider. Most agencies arrange delivery of hospital beds, oxygen equipment, and comfort medications within 24 hours of enrollment.
-
Connect with caregiver support resources immediately upon enrollment. Don’t wait until you feel overwhelmed to access respite care, support groups, or counseling services included in hospice benefits.
Understanding how to start hospice care at home provides additional detail for California families navigating this process. You can also explore comprehensive Graceland hospice care services to understand what professional support looks like in practice.
The enrollment process typically completes within 48 to 72 hours once physician certification is secured, allowing rapid access to symptom management and family support when you need it most.
Find compassionate hospice care in California with Graceland Hospice Care
Graceland Hospice Care delivers licensed, comprehensive end-of-life services throughout California, supporting families through every aspect of home-based hospice care. Our interdisciplinary team brings decades of combined experience in pain management, emotional support, and caregiver education, ensuring your loved one receives dignified, compassionate care aligned with their values and wishes.
We understand that reaching out for hospice support represents a profound decision. Our approach begins with listening to your family’s unique concerns, explaining options clearly, and developing personalized care plans that honor individual preferences. From initial assessment through bereavement support, we partner with families to reduce suffering and create meaningful time together.
Explore our Graceland hospice care programs and comprehensive Graceland hospice services that address medical, emotional, and practical needs throughout the end-of-life journey. Visit our Graceland Hospice Care home page or contact our team today for a free consultation that could transform your caregiving experience and your loved one’s comfort during this sacred time.
Frequently asked questions about end-of-life care and hospice in California
When should we consider hospice care for a terminally ill loved one?
Consider hospice when a physician indicates your loved one has six months or less to live if their illness progresses normally, and when curative treatments no longer provide benefit or cause more harm than good. Earlier referral allows maximum time to benefit from symptom management, caregiver education, and emotional support services.
What is the main difference between hospice and palliative care?
Hospice requires a terminal prognosis of six months or less and focuses exclusively on comfort without curative treatments, while palliative care can be provided at any serious illness stage alongside treatments aimed at cure. Both prioritize symptom relief and quality of life, but differ in timing and treatment approach.
What support does hospice provide for family caregivers?
Hospice offers comprehensive caregiver support including hands-on training for medication administration and patient care, 24-hour nurse access for questions and crises, respite care allowing caregiver breaks, counseling services addressing emotional strain, and bereavement support continuing 13 months after death. This education reduces caregiver anxiety and depression by 30-40%.
Will hospice care help my loved one live longer or hasten death?
Hospice care does not hasten death and may actually extend life by preventing complications, reducing harmful hospitalizations, and providing superior symptom management that keeps patients stronger. The focus on comfort rather than aggressive interventions allows natural disease progression without treatment side effects that often shorten survival.
How do I start the conversation about hospice with our doctor?
Ask your physician directly, “Do you think my loved one’s prognosis qualifies for hospice care?” or “Would hospice services improve comfort and quality of life at this stage?” Request a formal prognosis assessment if the doctor seems uncertain. Bring specific concerns about pain control, frequent hospitalizations, or declining function to illustrate why you’re considering this option.
Does Medicare or insurance cover hospice care costs in California?
Medicare covers hospice care completely when eligibility criteria are met, including all medications for symptom management, medical equipment, team visits, and respite care. Medicaid and most private insurance plans also provide comprehensive hospice coverage with little to no out-of-pocket cost to families, removing financial barriers to accessing compassionate end-of-life support.
Recommended
- Role of Caregivers in Hospice – Making End-of-Life More Compassionate | Graceland Hospice Care Blog
- What Is End of Life Care? Choices for Families | Graceland Hospice Care Blog
- Caregiver Support in Hospice: Easing End-of-Life Care | Graceland Hospice Care Blog
- End of Life Care Guide for Compassionate At-Home Support | Graceland Hospice Care Blog
- What Is Sleep Support and Why It Matters – Asli Nutrition